
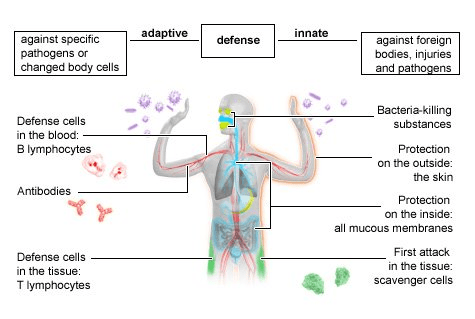
The immune response is crucial to preventing infection, promoting wound healing, and maintaining your body’s internal equilibrium. The overall immune response consists of 2 distinct immune systems – the innate immune system and the adaptive immune system. The innate immune response is the first to react to the infiltration of a pathogen or onset of a wound. Let’s dive into the complexities of the innate immune response!
The first aspect to understand about innate immunity is that it’s a layered response. For instance, let’s say you wipe your finger with alcohol wipes before biting your finger nail off. Since you wiped the area first, there is likely only a small bacterial load that entered the open skin. This means that the amount of inoculation is very little, which would result in a very minor infection. To combat the infiltration of pathogens, you have non-specific effector cells located in the skin. These effector cells are part of the innate immune system and are responsible for swiftly removing the pathogens that enter the body. Remember that non-specific immune cells, which are cells that will attack any pathogen, are always a part of the innate immune system. Innate immunity is defined by non-specific quick attacks. Given that there is only a minor infection and there are proximal effector cells, which can swiftly eliminate the pathogens, there will be no redness or swelling.
On the other hand, if you ripped you nail off after only rinsing it with water, the infiltrating bacterial load is of a medium amount, resulting in a greater inoculum than before. To combat this larger infection, you will still need the innate immune system, but a more complex innate immune response will be initiated given the more significant infection. First, the innate immune response recognizes microbial associated molecular patterns expressed by the pathogen. These patterns activate macrophages, a phagocytic innate immune cell, priming them to eliminate infection. These activated macrophages can then secrete factors that recruit more macrophages, dendritic cells, and in the case of a more severe infection, adaptive immune cells (T & B cells). Given that there was more infiltrating pathogen, there will be some redness and swelling. However, you have now stopped the infection from spreading!
What if the bacterial load is TOO HIGH? This could happen if you stuck your finger in a pile of dirt in your garden and then ripped your fingernail off. This would result in an enormous inoculum. Given the large size of the bacterial load, the innate immune system cannnot contain and eliminate the infection on its own. As a result, the pathogenic antigen is transported to the lymph nodes, which is where the T and B cells are waiting. By binding to the receptors on the T and B cells, the pathogen’s antigen stimulates the T and B cells to differentiate, priming them to combat the infection. These cells then migrate back to the finger (the wound site) to eliminate the infection.
What the previous three layered example tells us is that the innate immune system is crucial as your body’s first line of defense. Without it, any invading pathogen will fester an infection and take over the body. In contrast, the adaptive immune system takes time to activate, and for infections of low and medium severity, the adaptive immune system isn’t activated; the innate immune system is more than sufficient to handle these low/medium level infections by itself. The adaptive immune response is only initiated when a high severity infection occurs. This means that the innate immune system manages the virus before the more selective acquired immune system can take action. Therefore, the innate immune response is overall more important than the adaptive one since within it innate immunity, even the least severe and dangerous pathogens can kill you.
The second thing we need to address is how the innate immune system recognizes an invading pathogen. The innate immune system does not have the sophisticated antibodies and T-cell receptors of the acquired immune system, but it does have receptors that can recognize pathogens. It is important to note that these receptors are different from those used by T & B cells. Now, the specificity of the innate immune system is inherited from your genome. The full gene encoding the receptor is present and maintained in the cell. Therefore, this gene does NOT have to undergo somatic rearrangement, like in the adaptive immune system. These encoding genes are expressed by different types of innate immune cells. For instance, all macrophages have the same encoding genes, which means that all macrophages have the same receptors and recognize the same pathogenic pattern, which subsequently triggers the same immediate response. The same holds true for other types of innate immune cells, like dendritic cells. Remember, the hallmark of innate immune cells is that they interact with and recognize a range of foreign molecule structures.
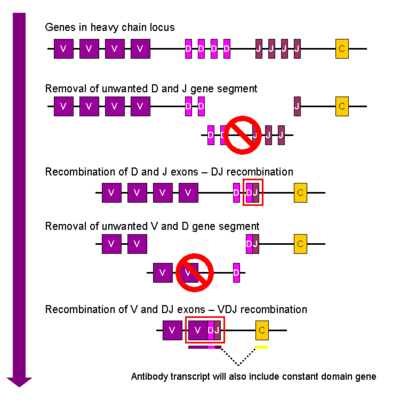
In contrast, the adaptive immune system is characterized by having a variety of cells, with each recognizing and targeting a different type of antigen. This means that one T cell does not interact with a range of molecule structures & and different foreign entities like one macrophage would. To create individual T and B cells that have targeted specificity towards one type of pathogen, there needs to be unique modifications to the genome present in each adaptive immune cell. Therefore, complicated somatic gene rearrangements of the adaptive immune system encoding genes occur, creating a unique genome for every T and B cell. A unique genome for every cell means that each B & T cell have distinct receptors on their surface and therefore, distinct specificities for one type of antigen.
The final aspect of innate immunity we need to discuss is the fixed barriers that innate immune system collaborates with to prevent the onset and spread of infection. The first barrier is the skin, and when intact, is very protective, preventing foreign pathogens from entering the body. The skin is a fixed barrier, so its ability to protect does not improve when exposed to an antigen. For instance, even if you wipe your skin with bacteria every day, it will not become better at protecting you from that specific bacteria. On the other hand, the adaptive immune system’s ability to protect you against a specific pathogen does improve upon antigenic exposure. This is the basis of vaccine biology and explains why getting a specific vaccine prevents you from getting smallpox or a severe case of the flu.
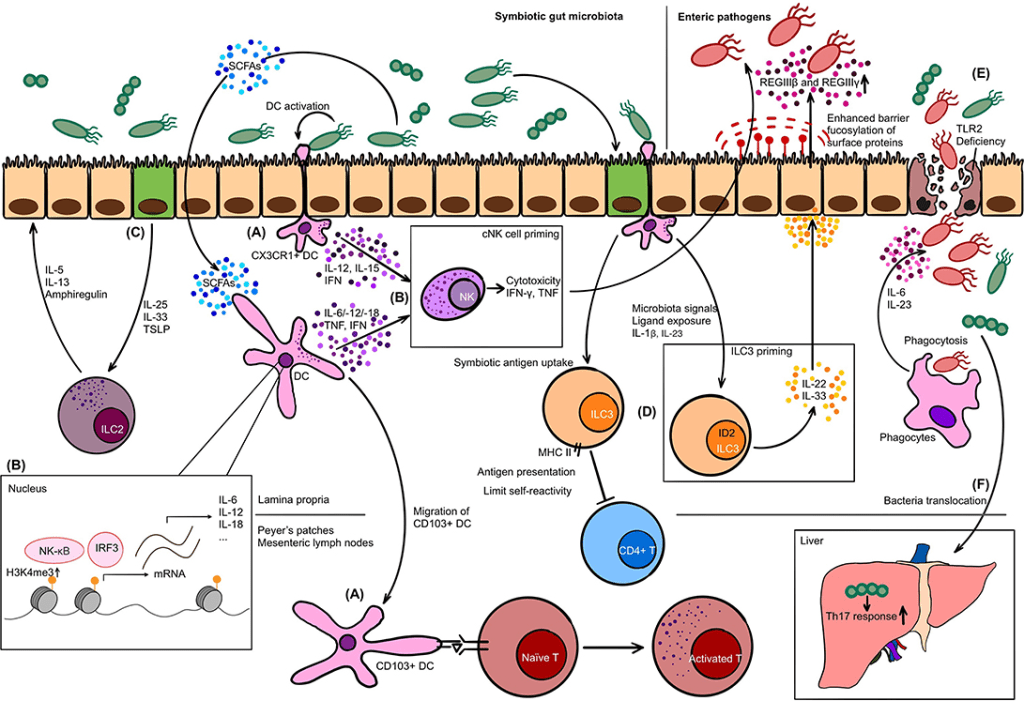
The lungs are also another fixed barrier that is crucial to the innate immune response. The lungs have cilia that continuously beat to clear any inhaled pathogens that we come in contact with. Additionally, the stomach plays a significant role as a pathogenic barrier. The high acid content in the stomach (low pH) destroys almost all bacteria that you would ingest. Commensal flora are also present in the gut, preventing our bodies from being overtaken by pathogenic bacteria. A great example of the role our gut microbiome plays in preventing infection is seen with antibiotics. When people are on antibiotics, which indiscriminately kills all bacteria, both the pathogenic bacteria they’re infected with and the bacteria composing the good gut microbiome are killed. When you finish taking the prescribed antibiotics, you will be more prone to being infected by other gastrointestinal (GI) infections because the gut flora is no longer present to protect that area.
In our next Immunology Blog, we will discuss the infectious process and how pathogens cause severe infections in the human body. See you next time!
